Saturday, 27 July, 2024
Tiny Nair
Some medical solutions work better “upside-down”. In 1930, in the sleepy Scottish town of Leith, Dr. Thomas Latta discovered a unique way of treating cholera: saltwater in a can, hung upside-down, connected to a tube, directly delivering its contents to the patient’s vein. Little did he know that his invention would not only save millions of lives but also save the skin of some house-surgeons in another part of the globe.
Working as a house-surgeon in a “free” government medical college in a north Indian metro was not easy, especially when the institution was situated in an area surrounded by an economically weak, labile and politically polarised population.
Jostling crowds, angry relatives, hypothyroid staff and overcrowded wards put the newly graduated house-surgeons in a precarious situation. The emotional trauma of disease and poverty, coupled with a lack of strong healthcare infrastructure, put tremendous pressure on the doctors, because to the public, the doctor is the face of medicine.
Shouting and verbal abuse were common and dismissed as irritants, and news of minor scuffles and skirmishes did not travel beyond the cafeteria table. Major violence, however, erupted once a week, on an average. Government medical hospitals have no real crowd control system, allowing anyone with the pretext of being a relative into the ward.
With medical knowledge covering only “exam-oriented” chapters and lots of mnemonics and hardly any hands-on experience, we foot soldiers were unarmed and our body language clearly gave it away to the relatives. With most senior faculty disappearing by sundown, we were supposed to fend for ourselves and our only advisers were the senior house-surgeons; their only additional qualification was that they had survived the ordeal for a year.
“If you see a sick, problematic patient and are unable to arrive at a provisional diagnosis, and you find more than half-a-dozen tough-looking relatives waiting for an answer, loudly announce that the situation looks serious and we have to investigate.” Our seniors taught us the first step of self-defence.
Statements such as “had the patient been brought a little earlier, we could have done better,” added punch. It mostly worked, except in special cases: The family of a patient, who was injured after a fall while climbing a coconut tree, lamented: “But sir, an hour earlier, he was eating breakfast at home…” Sometimes, the situation turned out to be more complex. It was then we needed to invoke Dr. Latta’s IV solution.
Back in the 1990s, starting an IV infusion and oxygen through nasal prongs always imparted a cinematic look to a doctor, somewhat appeasing bystanders. After setting up an IV “saline drip”, the most agitated bystander would be called and asked to watch the number of drops in the “see-through” drip-chamber.
This converted a potential troublemaker into a sheep-counting, sleep-deprived individual. Any subsequent deterioration in the patient’s condition could be blamed on the ‘drop-gazer’.
“A vial of B-complex injection, added to the IV fluid, imparts a canary yellow colour giving it a more authentic look,” a senior house-surgeon told us. And if there was a larger crowd, which was not happy with just the IV therapy, it was advised to “stand by” since “there may be need for blood donation”. The statement was made pointing to the menacing, tall, tough-looking guys.
This ensured a high bystander attrition rate, keeping the bedside clean, and getting appreciative looks from the consultant when he finally came for the rounds.
tinynair@gmail.com
-The Hindu

Do not make expressions casting dout on election: EC
14 Apr, 2022
CM Bhatta says may New Year 2079 BS inspire positive thinking
14 Apr, 2022
Three new cases, 44 recoveries in 24 hours
14 Apr, 2022
689 climbers of 84 teams so far acquire permits for climbing various peaks this spring season
14 Apr, 2022
How the rising cost of living crisis is impacting Nepal
14 Apr, 2022
US military confirms an interstellar meteor collided with Earth
14 Apr, 2022
Valneva Covid vaccine approved for use in UK
14 Apr, 2022
Chair Prachanda highlights need of unity among Maoist, Communist forces
14 Apr, 2022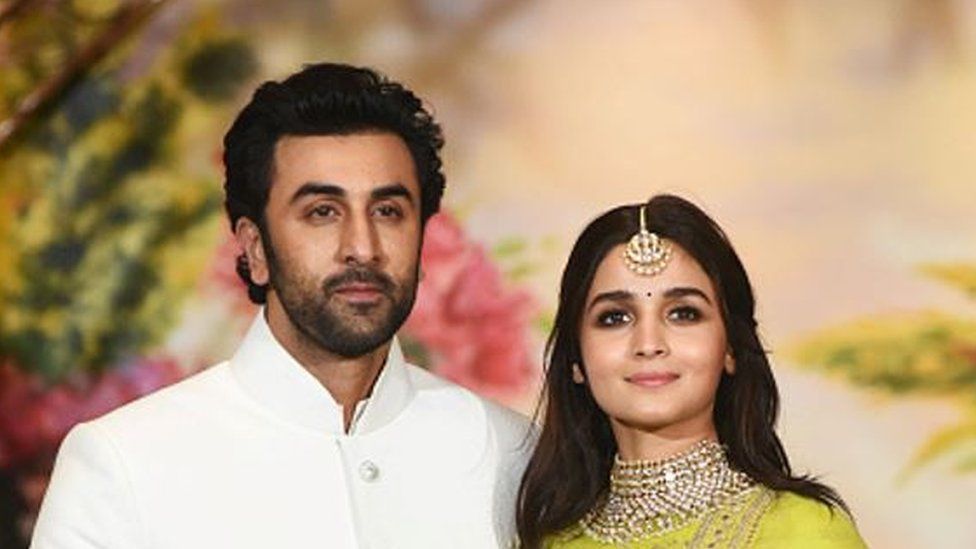
Ranbir Kapoor and Alia Bhatt: Bollywood toasts star couple on wedding
14 Apr, 2022
President Bhandari confers decorations (Photo Feature)
14 Apr, 2022